Tissue viability is everyone’s responsibility | Jacqui Fletcher Webinar
On Friday 24th July 2020, Jacqui Fletcher spoke at one of our popular Felgains Friday webinars. An Independent Nurse Consultant and Editor at Wounds UK, Jacqui is an expert in all things tissue viability.
During her session, she discussed the methods we could all use to ensure good skin management, as well as the role that mechanical turning systems, such as the VENDLET, have to play.
Let’s dive into some of the top learnings from her webinar.
The COVID-19 pandemic has brought opportunities, as well as challenges
One of the things that Jacqui had noticed throughout the COVID-19 crisis was how flexibility, creativity and innovation had emerged as key themes throughout the pandemic response. Health and care professionals have continued to provide high-quality care with “very few resources in very difficult scenarios”.
One example of this has been how colleagues have coped with the “blurring of boundaries” that has occurred due to COVID. Professionals have not only moved across geographical boundaries to help neighbouring health and care systems, or into new settings (for example, from acute into the community). But they have also coped with a blurring of boundaries between disciplines.
In an effort to slow the spread of the virus, patient contact between different health and care professionals has reduced. And this reduction in patient contact has meant that, although tissue viability has previously been firmly seen as a nursing role, other health and care professionals have by necessity become involved in pressure wound care and tissue viability work.
For instance, where podiatrists would have previously worked strictly below the ankle, many have been upskilled in compression bandaging for venous leg ulcers.
This widespread upskilling and broadening of responsibilities has been good news for patients, as professionals have been assessing patients’ needs beyond the boundaries of their own disciplines, and therefore in a more holistic way. And tissue viability and skin care have become everyone’s responsibility.
And as Jacqui mentions, the reason health and care professionals have been able to get involved in work traditionally undertaken by TVNs (Tissue Viability Nurses) has been down to the one common skill they all share: the ability to perform patient assessments. More on that later, but first…
What has traditionally been the work of a tissue viability nurse?
Although the average patient age is 75+, TVNs treat patients from cradle to grave: from premature babies to end-of-life patients. And despite the perception that leg and pressure ulcers are a disease of the elderly, they are increasingly affecting people in their 30s and 40s (many of whom are living with diabetes).
The most common wounds that TVNs treat are pressure ulcers – leg ulcers and diabetic foot ulcers. But they also treat complex surgical wounds, very deep wounds, wounds from amputation surgeries and fungating wounds, which occur during end-of-life.
TVNs also treat unusual skin conditions such as Steven Johnson syndrome, Bullous pemphigoid and other blistering diseases. Recently, they have also treated lesser-known COVID-19 symptoms which manifest themselves as skin conditions. For example, COVID toe, which to the eye looks very much like chilblains. A recent study by Casas et al. includes a very useful photo library of COVID skin manifestations.
So, how can we all be more engaged in tissue viability and skin care?
Whether you’re a patient, family member, therapist or support worker. There are two fundamental things we can all do to help manage skin care.
1. Undertake skin assessments
2. Review the patient’s mobility and activity
If these two things are done at every patient contact, we can all massively contribute to maintaining good skin health.
Skin assessments
In pressure sore prevention, the SSKIN framework is used:
S – Skin. Check the patient’s skin.
S – Surface. Check the surface that the patient is cared for on (a bed, chair etc.).
K – Keep the patient moving.
I – Increased moisture. People tend to think of this as incontinence, but it can also include moisture from sweat (recently patients with COVID-19 have had very high temperatures and have therefore produced a lot of sweat).
N – Nutrition and hydration.
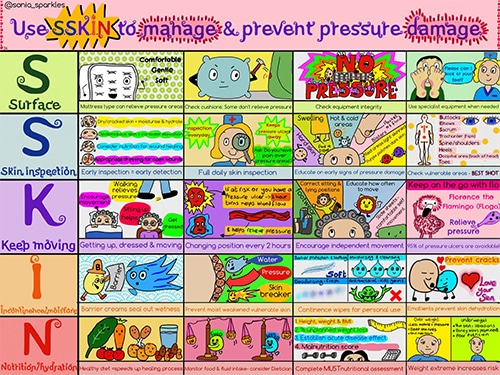
click on the image above to download this as a PDF
We can all carry out skin assessments by using our senses – but don’t just rely on what the skin looks like, use your sense of touch, too.
For example, the first sign of a pressure sore is inflammation. In pale skin, this can appear as a red spot that does not go white when pressed. However, this method of detection does not work as well with darker skin tones, so you must also use your sense of touch.
Is there an area of intense heat which is much warmer than the surrounding skin? This could indicate a category one pressure sore.
Or are there any areas that are very cold? That could be an indication that the skin has lost blood supply, which indicate much more serious damage.
In the lower limbs:
- Venous leg ulcers may exhibit dark brown staining of the skin
- Diabetic foot ulcers may be covered by calluses, which form on the skin to protect the underlying ulcer
- Swollen and heavy lower limbs can indicate oedema, which can impact upon the overall mobility of the patient, putting them at further risk, as mobility is key to the prevention of harm
Mobility and activity
When assessing a patient’s mobility and activity, remember that people can be immobile and still active. For example, a person who may be unable to walk could still be active in the upper body.
If these two assessments are carried out at every patient contact, we would all be doing our bit to prevent patient harm. And although a pressure ulcer is classed as a patient harm and is therefore a recordable incident, we must remember to consider the other reportable harms;
- Falls
- Leg clots
- Catheter-associated UTIs
When making assessments we need to ensure that we are considering the prevention of all of these patient harms holistically, and therefore not implementing solutions that may be successful in preventing one patient harm, but are hindering the prevention of another.
For example, using red socks to prevent falls, or anti-embolic socks to prevent leg clots may be putting the heels and feet at risk of skin damage.
So, make sure that objectives are not conflicting. The best way to do this is to consider all patient harms together and to communicate with all caregivers, including the families and patients themselves.
Carefully consider equipment solutions
Similarly, some common equipment solutions actually inhibit patient mobility and therefore increase the risk of pressure sores, leg clots and even catheter-related UTIs.
For example, if a specialist pressure mattress is installed which is very high, a wheelchair-user may find it difficult to get in and out of bed. In the same way, a stroke patient may struggle to enter and exit the bed if the edges of their specialist mattress are unstable. This reduces the opportunity to mobilise and actually increases their risk of patient harm.
Repositioning – communication is key
Do your repositioning timings complement the work that other health and care professionals are doing with the patient, or are your schedules/actions conflicting?
Timing is important.
For instance, if a patient is due to be repositioned, but the therapist has just been and the patient has spent a period being active and mobile, do they need to be repositioned as planned?
It’s OK to stray from set plans and schedules if that’s what’s best for the patients – just make sure that changes are accurately documented and communicated.
Mechanical and automated turning systems
Mechanical and automated turning systems are perfect for cases where:
- there are fewer people around (this has especially been the case during COVID where patient contact has been reduced for infection prevention reasons)
- patients have problems being manually handled (for example if they are confused, agitated or violent due to dementia or sedation, or find being manually handled painful and distressing)
Both mechanical and automated turning systems are good tools for these scenarios. However, as Jacqui points out, if we were to wholly rely on automated systems, we lose the opportunity for clinical assessment. And that human assessment is critical, as we need to continually check for moisture, redness and other discolouration and changes in skin temperature.
VENDLET Patient Turning Systems
VENLDET Patient Turning Systems allow a less intrusive “hands-off” approach to patient turning. This requires almost zero manual handling, and is much more dignified for the patient and can help reduce anxiety. The smooth, controlled motion and even distribution of pressure can also make repositioning more tolerable for patients in severe pain.
What to consider when repositioning patients in bed
- Are the pillows you’re using doing a good job?
If you’re manually repositioning a patient in bed, do you have the tools you need? For example, if you’re using pillows, do you have enough? Are they good enough quality and keep their shape? Or does the content spill to the sides and therefore lose the structural support you need to maintain a good position?
If so, you need LEJRELET repositioning aids.
LEJRELET cushions are made of viscoelastic foam which will not lose their shape, and therefore provide unbeatable postural support. They’re also coated in a vapour-permeable coating, which will help prevent a build-up of moisture – one of the 5 things Jacqui mentioned to watch out for as part of a skin assessment.
Learn more about LEJRELET positioning cushions.
- Keep the patient’s knees bent
If you’re lifting a leg by the ankle in order to offload pressure from the heels, make sure that you don’t hyper-extend the knee. This can simply be done by ensuring the knee is always bent a little.
- Under, or over 30-degree elevation?
Tissue viability nurses don’t like the head of the bed to be elevated above 30 degrees, as this can cause the patient to slide down the bed, which in turn causes shear damage. However, patients with chest or respiratory conditions, such as COVID-19, may require an elevation of 30+ degrees.
In situations like these where there are conflicting objectives, work with colleagues to identify priorities for the patient.
What to consider when repositioning patients in chairs
Specialist companies, like us here at Felgains, can provide chairs that can tilt-in-space. Tilt-in-space holds the user in a fixed position when in recline with the angle of the hip and the back remaining constant. This avoids any sliding forward in the chair and redistributes weight over a larger surface area to reduce the likelihood of pressure ulcers.
Using pillows, or even better – specialist postural supports, such as the LEJRELET support cushions, can ensure good posture, which helps to distribute weight and therefore pressure.
To conclude – everyone who sees a patient should be able to complete a skin assessment and a review of mobility and activity.
If everyone who came into contact with patients did these two things, patient harms such as pressure sores, falls, leg clots and catheter-related UTIs could be prevented.
If you’d like to discuss how our equipment solutions could help prevent pressure damage, please give one of our knowledgeable team members a call: 01473 741 144.
Or check out our range of pressure relief equipment online:
Reuben Bush
Reuben joined the Felgains team in August 2019, bringing with him passion and experience in marketing and design – from a rather different sector. His focus is now on improving each and every touchpoint of our customer experience and building a vast following of raving fans! He loves road cycling, and also happens to have rather a weakness for food – he’s a bona fide chocoholic!
